Heather Tanana**
I. Introduction
II. A Look at the Past To Understand the Present
A. Federal Policies and the Perpetuation of Historical Trauma
B. A Brief History of Mental Health and Health Services in Tribal Communities
III. The Impact of COVID-19 on Tribal Communities and Response To Facilitate Mental Health Services
A. COVID-19
B. Adapting To Address the Mental Health Needs of Tribes Through Telehealth Services
IV. Conclusion
The United States’ response to the coronavirus pandemic has been widely criticized.[1] The federal government failed to provide leadership and to fully appreciate the seriousness of the virus until it had reached all corners of the country. For many Americans, the lack of federal leadership may not have had a direct impact on their access to health care during this time. However, Tribal communities[2]generally rely on the federal government for their health care services.[3] When COVID-19 hit, it was not surprising that it devastated Tribal communities.[4] Based on past federal policies, American Indians and Alaska Natives suffer various health and socioeconomic disparities that make them not only more vulnerable to contracting COVID-19, but also more susceptible to negative outcomes once infected.[5]
Much attention has focused on COVID-19 infection rates and related deaths in Indian country.[6] The Navajo Nation experienced one of the highest infection rates in the country with more than 11,030 positive cases and at least 574 confirmed deaths.[7] However, the pandemic’s reach has gone beyond physical impacts on the body. COVID-19 has also affected the mental health of Tribal members and their access to mental health services.[8]
This Article dives into the effects of the coronavirus pandemic on the mental health and general well-being of Tribal communities. Part II sets the stage by providing the history of federal and Tribal relations, followed by a summary of the current state of mental health in Indian country. Part III discusses the impacts of COVID-19 and the rise of telehealth to provide much needed mental health services during the pandemic. The Article concludes by providing recommendations to continue the progress made to fill the historic gap in mental health services in Indian country post-pandemic.
II. A Look at the Past To Understand the Present
Federal policies have shaped the landscape in Indian country, leaving a lasting effect on the well-being of Tribal communities. To fully understand the impacts of COVID-19, this Part provides background on the federal policies affecting Tribes and their members, followed by a summary of the mental health issues facing Native Americans prior to the pandemic.
A. Federal Policies and the Perpetuation of Historical Trauma
The United States has a complex relationship with Native Americans that is defined by power disparity and unique historic legal arrangements. As the original inhabitants of this country, Tribes predate formation of the United States. In a series of cases known as the Marshall trilogy, the United States Supreme Court recognized Tribes’ inherent sovereignty to govern their own people and land—while ensuring that Tribes remained subservient to the federal government. [9] These cases established key (often competing) concepts and principles in federal Indian law—e.g., sovereignty, domestic dependent nations, and the trust relationship. Tribal sovereignty essentially is a Tribe’s right to govern itself.[10] And yet, Tribes are also domestic dependent nations, reliant upon the federal government for protection.[11] As a result, a trust relationship exists between the federal government and Tribes.[12] Comparisons have frequently been made to a relationship like that of a guardian and ward, or a trustee and beneficiary.[13] The federal government has a duty to protect Tribal rights.[14] Always hovering in the background is Congress’s absolute right to extinguish any and all Tribal rights, including the very existence of Tribal nations in this country.[15] However, “[u]nless and ‘until Congress acts, the tribes retain’ their historic sovereign authority.”[16]
The challenge of balancing the rights of Tribes against those of the federal government has an unbalanced history. At times, the federal government appears to have simply not wanted to go through the effort. The pervasive belief that Native Americans should adopt the white man’s ways and be incorporated into the general U.S. population led to federal policies that had severe consequences on Tribes and their members, including the termination of Tribal status and cultural identity.[17] Even when the federal government tolerated Tribes, other federal policies—such as the Reservation Era—still had a negative impact on the general well-being and success of Native Americans.[18] It was not until the most recent era—the Indian Self-Determination Era—that the federal government truly embraced Tribal existence and their inherent right to self-governance.[19] Nonetheless, to this day, federal actions are frequently taken to undermine or disregard Tribal sovereignty.[20]
A basic understanding of the various federal policies is essential to understanding the current landscape in Indian country. Accordingly, a brief summary of the Indian federal policies is provided below:[21]
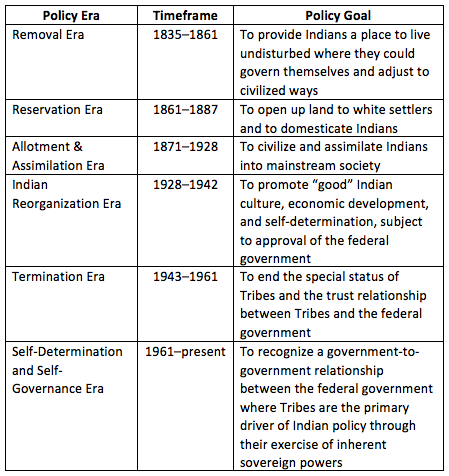
Other scholarship discusses the Indian federal policies in more detail.[22] For purposes of this article, it is sufficient to understand that the federal government has not always been a friend to Tribes and at times has taken action directly contrary to Tribal sovereignty and the general well-being of Native Americans. Such actions have resulted in historical trauma that perseveres today.[23]
Historical trauma is defined as “cumulative emotional and psychological wounding across generations, including the lifespan, which emanates from massive group trauma.”[24] Historical trauma has been connected to depression, anxiety, suicidality, and substance abuse.[25] Understanding historical trauma is essential when working with Native communities. And yet, it can be a challenging concept to fully grasp if you have not experienced it. To help illustrate this important concept, I often share pieces of my own family history and the influence past events experienced by my ancestors have had on my life:
My great grandmother was a small child when she and her family were forced to leave the only home she had ever known. They walked over 300 miles with the Army pushing them along with the point of a rifle in what is known today as the Long Walk. I never met my great grandmother. She had passed on to the afterlife long before I was born. And yet, I think of what she survived often. I imagine that she was confused and did not understand why their home and belongings were burned to the ground. I envision her with her head held high, attempting to mirror her own mother, and pretending to be brave despite the harsh sun blinding her eyes and blisters forming on her feet. Did her mother attempt to shield her from the dead bodies that seemed to increase in number each day? Or had they become accustomed to seeing death by then, something not to be spoken about in accordance with Diné culture?
My father was stolen from his mother. When the government agent showed up unannounced and took him, my grandmother did not know if she would ever see my father again. My father was taken to a boarding school to be educated hundreds of miles away. Foreign words flew over his head. When he asked for help in the only language he knew, he was beaten. To this day, I tear up every time I think of how scared and alone he must have felt. I double check to make sure that I locked my doors so that no one will sneak in during the night to take my children.
I grew up in a safe home with two loving parents. I have experienced privilege in knowing that I would never go to bed hungry or lack a roof over my head. And yet, my heart aches for what my ancestors experienced. I feel anxious and cannot forget their pain. That is historical trauma.
My ancestors’ experiences and the aftermath are not unique among Native people. In light of its widespread prevalence, those working with Tribal communities must acknowledge the continued existence of historical trauma and its impacts.
B. A Brief History of Mental Health and Health Services in Tribal Communities
“The disproportionate rates of mental and behavioral health issues faced by Native Americans have been attributed in part to the ongoing impact of historical trauma.”[26] Native Americans suffer from high rates of alcohol and substance abuse, mental health disorders, suicide, violence, and behavior-related chronic diseases.[27] Native Americans experience serious psychological distress at a rate of 2.5 times more than the general population.[28] Native youth have suicide death rates more than double that of non-Hispanic whites[29] and also use and abuse alcohol and other drugs at younger ages and higher rates than other groups.[30] The life expectancy for Native Americans is 5.5 years less than the national average.[31] Native elders are particularly vulnerable. Elders play a revered role in Tribal communities as the gatekeepers of traditional knowledge and culture.[32] But research suggests that based upon the high prevalence of depression and dementia among Native elders, immediate action is required to avoid an epidemic.[33] Legitimate concerns about elder abuse, neglect, and maltreatment also prompted the Navajo Nation to pass the Diné Elder Protection Act.[34]
Stemming from treaty obligations, the federal government is primarily responsible for providing health services to Native Americans.[35] This obligation has been interpreted to be a part of the federal government’s trust responsibility to Tribes.[36] Various federal laws have been passed that affect the general welfare of American Indians and health services received; however, a few have been instrumental in establishing the status quo and deserve to be noted: the Snyder Act, Indian Self-Determination and Education Assistance Act (ISDEAA), and Indian Health Care Improvement Act (IHCIA).[37]
The Snyder Act of 1921 first authorized funds for the “relief of distress and conservation of health” of American Indians, including the employment of physicians.[38] Originally, the Bureau of Indian Affairs, under the Department of Interior, was the responsible federal agency, but this role transferred to the Department of Health and Human Services (HHS), and the Indian Health Service (IHS) was created.[39] The mission of IHS is “to raise the physical, mental, social, and spiritual health of American Indians and Alaska Natives to the highest level.”[40]
The ISDEAA was enacted during the Self-Determination and Self-Governance Era.[41] The Act allowed Tribes to enter into agreements with IHS to assume management of health-related programs and services.[42] Under such agreements—often referred to as 638 compacts or contracts—Tribes are able to tailor programs and services to their community needs.[43]
Originally passed in 1976,[44] the IHCIA was permanently reauthorized in 2010.[45] The IHCIA confirmed the federal government’s responsibility to improve the health of Native Americans, allocated additional resources for health services, and established Urban Indian Health Programs.[46] Today, the health care delivery system is known as the “I/T/U” system and refers to three different means of service: “I” for IHS; “T” for Tribal programs under the ISDEAA; and “U” for urban health centers. For many Native Americans, the I/T/U system is the only source of health care, including mental health services.[47]
While the federal government has acknowledged its responsibility to provide health services, Congress has historically failed to appropriate sufficient funding to meet the health-related needs of Native Americans.[48] IHS health care expenditures are approximately 1/3 of those for federal health care spending nationwide.[49] “Indeed, when adjusted for inflation and population growth, the IHS budget has remained static in recent decades, with little additional funding available to target the chronic health disparities facing Native communities.”[50] To help fill this funding shortfall, IHS has turned to third-party revenue by billing a patient’s private insurance or the Centers for Medicare & Medicaid Services (CMS) when applicable.[51]
Mental health services in particular lack infrastructure support.[52] The IHS Mental Health “program is a community-oriented clinical and preventive service program” that focuses on providing acute, crisis-oriented outpatient services.[53] Over half of the mental health budget and associated programs are managed directly by Tribes under the ISDEAA.[54] Regardless of the delivery system—IHS or Tribally operated—health facilities serving Tribal communities often lack skilled and trained personnel, including psychiatrists and psychologists due to the remote location.[55] Their geographic isolation also makes it challenging to refer individuals from Tribal communities to resources located off reservations.
III. The Impact of COVID-19 on Tribal Communities and Response To Facilitate Mental Health Services
Before COVID-19 spread to Indian country, Tribal communities faced significant challenges, including health and socioeconomic disparities.[56] For example, many Tribal members lack running water and electricity.[57] Households are often overcrowded, sharing a small amount of space with multiple generations.[58] Further, the rhythms of life in many rural Tribal communities exacerbate potential transmission points. Tribal members typically have to travel long distances to shop at the only grocery store available.[59] Because going to the store is an event that takes several hours and provides social interaction, families often shop together.[60] Add to this a lack of running water, and the risk of COVID transmission is counter-intuitively exacerbated by the remote landscape of Tribal communities. Finally, as discussed in more detail below, many Native Americans suffer from pre-existing conditions—like diabetes, hypertension, obesity, heart disease, alcoholism, asthma—that exacerbate the risks of contracting COVID.[61] These existing conditions have a direct effect on the virus’s impact in Tribal communities. This Part discusses the impact of COVID-19 on Native Americans and the use of telehealth services to provide mental health services during the pandemic. It concludes with lessons learned and recommendations for after the pandemic ends.
The Center for Disease Control (CDC) recently released a report on the incidence of COVID-19 among Native Americans.[62] The CDC found the overall COVID-19 incidence rate among Native Indians to be 3.5 times higher than that of white persons.[63] The report noted that several factors play into this disparity. “Historical trauma and persisting racial inequity have contributed to disparities in health and socioeconomic factors between AI/AN and white populations that have adversely affected AI/AN communities; these factors likely contribute to the observed elevated incidence of COVID-19 among the AI/AN population.”[64] Shared transportation, limited access to running water, household size, and other factors prevalent in Tribal communities also may facilitate COVID-19 community transmission.[65] Once infected, Native American adults have the highest risk of developing severe illness compared to other groups.[66] While data gaps exist,[67] the current available data clearly shows that Tribal communities have been hit hard.[68]
The full impact of COVID-19 on mental health is the subject of ongoing study and will not be known until after the pandemic ends. However, research has shown that large-scale disasters, whether traumatic, natural, or environmental, “are almost always accompanied by increases in depression, posttraumatic stress disorder (PTSD), substance use disorder, a broad range of other mental and behavioral disorders, domestic violence, and child abuse.”[69] Social isolation, loneliness, and job loss—all consequences of the pandemic—have also been linked to poor mental health, including increased depression, anxiety, substance abuse and suicide.[70]
Tribal communities are generally close knit with frequent opportunities for social interaction through traditional gatherings. While research is not yet available specific to American Indians and Alaska Natives, a Canadian survey sheds some light on the impact of social isolation within Indigenous communities. A survey in Canada showed that sixty percent of Indigenous respondents felt their mental health had worsened since the onset of the pandemic and social distancing measures.[71] Overall, higher proportions of Indigenous participants reported worsened mental health since the pandemic than non-Indigenous participants.[72] First Nations people in Canada share a similar history of colonization and systemic inequalities to Native Americans in the United States.[73] Given the similarities, it is reasonable to assume that the mental health of American Indians and Alaska Natives has also been disproportionately impacted during the pandemic.
B. Adapting To Address the Mental Health Needs of Tribes Through Telehealth Services
Three actions have been suggested to address the increase in mental health conditions associated with the pandemic.[74] First, digital technologies should be used to bridge social distance and ameliorate loneliness.[75] Second, mechanisms for surveillance, reporting, and intervention should be implemented.[76] And, finally, stepped care should be provided by utilizing the most effective, least resource-heavy treatment first and then following with more resource-heavy treatment based on patients’ needs.[77]
Telehealth—the use of electronic communications for health care—can support all three of these protective measures. Outreach and screening for loneliness and associated mental health conditions can be conducted through telehealth services and existing reporting and intervention measures adopted. Mental health visits, group visits, and other care via technology platforms can also provide acute crisis management and routine communication and support.
There are three main types of telehealth services:
(1) Telehealth visits provide services that generally occur in-person;
(2) Virtual check-ins are brief communications with providers and their established patients to determine whether an office visit or other service is necessary; and
(3) E-visits are communications between providers and their established patients through an online patient portal.[78]
Shifts in federal policy have paved the way for use of telehealth in Indian country. Prior to the pandemic, telehealth visits were not reimbursed by CMS or private insurance companies at the same rate as in-person medical services and were generally limited to rural areas.[79] This changed when the Secretary of HHS invoked § 1135 of the Social Security Act and issued a blanket waiver.[80] The Coronavirus Aid, Relief, and Economic Security (CARES) Act further broadened HHS’s authority to waive various CMS requirements in response to the pandemic.[81] The primary purpose of the waiver was to allow patients to have access to physicians and other clinicians while staying at home under safety orders and to mitigate spread of the virus.[82] Under the waiver, Medicare telehealth services are available to beneficiaries regardless of where they are located.[83] CMS requires most telehealth services to be implemented using technology with audio and video capabilities for two-way, real-time interactive communication.[84] But, the waiver allows the use of audio-only equipment to provide certain services, including behavioral health counseling.[85] The waiver also allowed for a broader range of practitioners to use telehealth to provide Medicare services. All health care practitioners who are authorized to bill Medicare for their professional services may also furnish and bill for telehealth services and may do so from any location during the pandemic.[86] Many private insurers have followed suit to cover telehealth services during the pandemic.[87]
The pandemic has created a unique opportunity to make advances in mental health service delivery in Tribal communities. Tribal communities historically have had limited access to care for behavioral health.[88] Telehealth services present a potential remedy to this problem and should continue to be supported and developed. To do so, CMS’s changes regarding telehealth services should be made permanent by Congressional action.
IHS must also be fully funded. IHS received a much needed surge of money from COVID-19 legislation packages.[89] And while funds can be used to improve teleworking capabilities,[90] there are restrictions on how and when the funds can be used.[91] Moreover, pre-pandemic, the IHS system was already overburdened and underfunded.[92] To fully fund IHS, an estimated $32 billion is required.[93] Congress must appropriate sufficient funds to IHS to allow it to fulfill its mission and the federal government’s treaty obligations.
IHS and Tribes should receive dedicated funding to build much needed infrastructure in Indian country. Greater infrastructure development is required to facilitate widespread implementation of telehealth services. Approximately thirty-five percent of Indian country residents lack access to broadband internet.[94] Growing attention to the lack of other utilities, such as public water systems and electricity, should be harnessed to develop a comprehensive infrastructure development plan in Indian country that includes greater access to cell phone and broadband services.
Finally, IHS and Tribally operated facilities should establish telehealth programs that incorporate the recruitment and training of mental health professionals to provide culturally appropriate telehealth services. Culturally competent care helps ensure that patients do not feel alienated or disrespected; and therefore are more likely to comply with treatment. Telehealth programs should also work with the community to promote acceptance of technology and use of telehealth services.
Prior to the coronavirus pandemic, Native Americans suffered health, social, and economic disparities that in large part were a result of past federal policies and broken promises. When COVID-19 spread to Tribal communities, these disparities exacerbated the spread and severity of the virus. Unsurprisingly, the data demonstrate that Tribal communities have been hit almost three times as hard as other communities. Though not yet thoroughly documented, this will also have a toll on mental health. While many will not come out of the pandemic unharmed, the pandemic has brought attention to the challenges Tribal communities face and provided a unique opportunity to address some of the historical inequities that exist. The expansion of telehealth services has offered one solution to providing greater access to mental health services in Tribal communities. We should continue to build off progress made during the pandemic to fully implement telehealth services permanently in Indian country.
* This paper was published in November 2020 during the COVID-19 pandemic. All dates and time descriptions refer to the 2020–21 COVID-19 pandemic unless otherwise stated.
** Heather Tanana is an Assistant Research Professor and Wallace Stegner Center Fellow at the University of Utah’s S.J. Quinney College of Law. She is also an Associate Faculty member at Johns Hopkins University’s Bloomberg School of Public Health. She is a citizen of the Navajo Nation.
[1]. See, e.g., Toluse Olorunnipa, Josh Dawsey & Yasmeen Abutaleb, With Trump Leading the Way, America’s Coronavirus Failures Exposed by Record Surge in New Infections, Wash. Post (June 27, 2020, 2:38 PM), https://www.washingtonpost.com/politics/with-trump-leading-the-way-americas-coronavirus-failures-exposed-by-record-surge-in-new-infections/2020/06/27/bd15aea2-b7c4-11ea-a8da-693df3d7674a_story.html [https://perma.cc/3A3L-EKBM].
[2]. In this article, the Indigenous populations of the United States are interchangeably referred to as American Indian and Alaska Natives (AI/AN), Native, Tribal, and Indian (the term largely used in federal law).
[6]. Simon Romero, Checkpoints, Curfews, Airlifts: Virus Rips Through Navajo Nation, N.Y. Times (Apr. 20, 2020), https://www.nytimes.com/2020/04/09/us/coronavirus-navajo-nation.html [https://perma.cc/EMT9-8PMC].
[7]. Dikos Ntsaaígíí-19 (COVID-19), Navajo Dep’t of Health (Oct. 21, 2020), https://www.ndoh.navajo-nsn.gov/COVID-19 [https://perma.cc/JBH8-6AUY].
[9]. The Marshall trilogy consists of the following three cases: 1) Johnson v. M’Intosh 21 U.S. (8 Wheat.) 543, 574 (1823) (stating Native Americans’ “rights to complete sovereignty, as independent nations, were necessarily diminished” because “discovery gave exclusive title to those [Europeans] who made it”); 2) Cherokee Nation v. Georgia, 30 U.S. (5 Pet.) 1, 17 (1831) (stating the Cherokee Nation was not a foreign nation but was rather a “domestic dependent nation”) (1831); and 3) Worcester v. Georgia, 31 U.S. (1 Pet.) 515 (1832) (affirming the principle that the federal government alone has authority over Indian Affairs).
[10]. See, e.g., Cherokee Nation, 30 U.S. (1 Pet.) at 4 (“[T]he Cherokee nation[ ] and the other nations have been recognized as sovereign and independent states; possessing both the exclusive right to their territory, and the exclusive right of self government within that territory.”).
[11]. Id. at 17 (“They [Native Americans] look to our government for protection.”).
[12]. The trust relationship between the federal government and Tribes is well established. See, e.g., Cohen’s Handbook of Federal Indian Law § 4.01 (Nell Jessup Newton ed., 2017) [hereinafter Cohen’s Handbook] (discussing “tribal power to impose a variety of taxes . . . on tribal or trust land”).
[13]. See, e.g., Cherokee Nation, 30 U.S. (1 Pet.) at 17 (“Their relation to the United States resembles that of a ward to his guardian”).
[14]. See, e.g., Cohen’s Handbook, supra note 12, § 4.01 (citing Ex parte Crow Dog, 109 U.S. 556, 568 (1883) (stating the United States had a duty to protect the tribe’s right to self-government)).
[15]. Matthew L.M. Fletcher, A Short History of Indian Law in the Supreme Court, 40 A.B.A. Hum. Rts. Mag. (Oct. 1, 2014), https://www.americanbar.org/groups/crsj/publications/human_rights_magazine_home/2014_vol_40/vol–40–no–1–tribal-sovereignty/short_history_of_indian_law/ [https://perma.cc/7JSF-46LV].
[16]. Michigan v. Bay Mills Indian Cmty., 572 U.S. 782, 788 (2014) (quoting United States v. Wheeler, 435 U.S. 313, 328 (1978)).
[17]. See e.g., Stephen Pevear, The Dawes Act: How Congress Tried To Destroy Indian Reservations, Oxford U. Press Blog (Feb. 8, 2012), https://blog.oup.com/2012/02/dawes-act-congress-indian-reservations/ [https://perma.cc/H82J-K49J].
[18]. See e.g., Leslie Sanchez et al., The Economics of Indigenous Water Claim Settlements in the American West, 15 Env’t Rsch. Letter 1, 9–10 (2020), https://iopscience.iop.org/article/10.1088/1748-9326/ab94ea/pdf [https://perma.cc/485R-6TM8].
[19]. Geoffrey D. Strommer & Stephen D. Osborne, The History, Status, and Future of Tribal Self-Governance Under the Indian Self-Determination and Education Assistance Act, 39 Am. Indian L. Rev. 1, 16–18 (2015).
[20]. See e.g., Carl Slater, Opinion, Lezmond Mitchell’s Death Sentence Is an Affront to Navajo Sovereignty, N.Y. Times (Aug. 19, 2020), https://www.nytimes.com/2020/08/19/opinion/lezmond-mitchell-death-sentence-execution.html [https://perma.cc/Y54S-EQE8].
[21]. See generally Justin Blake & Sarah Deer, Introduction to Tribal Legal Studies 82–101 (3rd ed. 2016); Cohen’s Handbook, supra note 12, § 1.
[22]. See e.g., Cohen’s Handbook, supra note 12, § 1.
[24]. Maria Yellow Horse Brave Heart et al., Historical Trauma Among Indigenous Peoples of the Americas: Concepts, Research, and Clinical Considerations, 43 J. Psychoactive Drugs 282, 283 (2011).
[26]. U.S. Comm’n on C.R., Broken Promises: Continuing Federal Funding Shortfall for Native Americans 77 (2018), https://www.usccr.gov/pubs/2018/12-20-Broken-Promises.pdf [https://perma.cc/NZF7-QYR6].
[27]. Fact Sheet: Behavioral Health, Indian Health Serv. (Oct. 2016), https://www.ihs.gov/newsroom/factsheets/behavioralhealth/ [https://perma.cc/CBQ4-PEVY].
[28]. Nat’l Ctr. for Health Stats., U.S. Dep’t of Health & Human Servs., Health, United States, 2017: With Special Feature on Mortality tbl.46 (2017), https://www.cdc.gov/nchs/data/hus/2017/046.pdf [https://perma.cc/TLY3-WV4X] (showing 3.6% percent of American adults experienced serious psychological distress in the previous thirty days whilst American Indians of the same category experienced the same at a rate of 9.2%).
[29]. Rachel A. Leavitt et al., Suicides Among American Indian/Alaska Natives—National Violent Death Reporting System, 18 States, 2003–2014, 67 Morbidity & Mortality Wkly. Rep. 237, 239 (2018).
[30]. Am. Psychiatric Ass’n, Mental Health Disparities: American Indians and Alaska Natives 2 (2017), https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-American-Indian-Alaska-Natives.pdf [https://perma.cc/EXS8-6DN7].
[31]. Fact Sheet: Disparities, Indian Health Serv., (Oct. 2019) https://www.ihs.gov/newsroom/factsheets/disparities/ [https://perma.cc/Q248-GPJ2].
[32]. Substance Abuse & Mental Health Servs. Admin. et al., The National Tribal Behavioral Health Agenda 11 (2016), https://www.samhsa.gov/sites/default/files/topics/tribal_affairs/national-tbha-ai-an-communities-draft.pdf [https://perma.cc/YA9U-HCXX].
[33]. Mario Garrett et al., Mental Health Disorders Among an Invisible Minority: Depression and Dementia Among American Indian and Alaska Native Elders, 55 Gerontologist 227, 228 (2015).
[34]. 9 Navajo Nation Code §§ 1801–1817 (2020), http://www.navajocourts.org/Tit9.htm#ELDER [https://perma.cc/5DSW-YWNA].
[35]. See Fact Sheet: Basis for Health Services, Indian Health Serv. (Jan. 2015), https://www.ihs.gov/newsroom/factsheets/basisforhealthservices/ [https://perma.cc/6RJW-HJHV] (discussing the “legal basis for the federal obligation to provide health care to American Indians”).
[36]. See Indian Health Care Improvement Act, 25 U.S.C. §§ 1601–1685.
[37]. See Donald Warne & Linda Bane Frizzell, American Indian Health Policy: Historical Trends and Contemporary Issues, 104 Am J. Pub. Health 263, 263 (2014) (discussing the existing federal laws impacting AI/AN populations and conditions necessary to ensure improved AI/NA health).
[39]. Transfer Act, Pub. L. No. 83-568, 68 Stat. 674 (1954).
[40]. About IHS, Indian Health Servs., https://www.ihs.gov/aboutihs/ [https://perma.cc/LNH9-G9MT].
[41]. Indian Self-Determination and Education Assistance Act, Pub. L. No. 93-638, 88 Stat. 2203 (enacted in 1975).
[43]. Off. of the Inspector Gen., Dep’t of Health & Hum. Servs., Tribal Contracting for Indian Health Services 1 (1996), https://oig.hhs.gov/oei/reports/oei-09-93-00350.pdf [https://perma.cc/PF6M-JMA6].
[44]. Indian Health Care Improvement Act, 25 U.S.C. §§ 1601–1680.
[45]. Permanent Authorization of the IHCIA was part of the Patient Protection and Affordable Care Act, Pub. L. No. 111–148, 124 Stat. 119, 935.
[47]. U.S. Comm’n on C.R., supra note 26, at 64.
[55]. See Id. at 69; Erin Bagalman & Elayne J. Heisler, Cong. Rsch. Serv., R44634, Behavioral Health Among American Indian and Alaska Natives: An Overview 9 (2016), https://fas.org/sgp/crs/misc/R44634.pdf [https://perma.cc/79YP-MCGJ].
[56]. Aila Hoss & Heather Tanana, Upholding Tribal Sovereignty and Promoting Tribal Public Health Capacity During the COVID-19 Pandemic 78 (Univ. of Utah Coll. of L., Working Paper No. 391, 2020), https://ssrn.com/abstract=3675940 [https://perma.cc/25AJ-2WEV].
[59]. See, e.g., Amelia Nierenberg, For the Navajo Nation, a Fight for Better Food Gains New Urgency, N.Y. Times (Aug. 3, 2020), https://www.nytimes.com/2020/08/03/dining/navajo-nation-food-coronavirus.html [https://perma.cc/HDM2-6FHX]; Emily M. Piltch et al., The Complexities of Selling Fruits and Vegetables in Remote Navajo Nation Retail Outlets: Perspectives from Owners and Managers of Small Stores, 23 Pub. Health Nutrition 1638, 1639 (2020).
[60]. COVID-related educational material has stressed the importance of shopping alone rather than as a group. Essential Shopping Tips, Navajo Health Command Operation Ctr., https://www.ndoh.navajo-nsn.gov/Portals/0/COVID-19/News/shop.pdf?ver=QaHn5RN3CbzkNISu747C9A%3d%3d [https://perma.cc/CK7T-XVKC].
[62]. Sarah M. Hatcher et al., COVID-19 Among American Indian and Alaska Native Persons—23 States, January 31–July 3, 2020, 69 Morbidity & Mortality Wkly. Rep. 1166 (2020).
[63]. Id. at 1167. Notably, the CDC report likely underestimates the actual COVID-19 incidence among Native Americans based upon data limitations. Id. at 1167–68.
[64]. Id. at 1167.
[66]. Wyatt Koma et al., Low-Income and Communities of Color at Higher Risk of Serious Illness if Infected with Coronavirus, Kaiser Fam. Found. (May 7, 2020), https://www.kff.org/coronavirus-covid-19/issue-brief/low-income-and-communities-of-color-at-higher-risk-of-serious-illness-if-infected-with-coronavirus/ [https://perma.cc/2KC4-TBPL].
[67]. See Aila Hoss, Exploring Legal Issues in Tribal Public Health Data and Surveillance, 44 S. Ill. U. L.J. 27 (2019) (discussing Tribal public health data and challenges).
[68]. See Hatcher, supra note 62.
[69]. Sandro Galea, Raina M. Merchant & Nicole Lurie, Opinion, The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention, 180 JAMA Internal Med. 817, 817 (2020).
[70]. Nirmita Panchal et al., The Implications of COVID-19 for Mental Health and Substance Use, Kaiser Fam. Found. (Aug. 21, 2020), https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use/ [https://perma.cc/B7TS-DA28].
[71]. Paula Arriagada, Tara Hahmann & Vivian O’Donnell, Indigenous People and Mental Health During the COVID-19 Pandemic, Stat. Can. (June 23, 2020), https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00035-eng.htm [https://perma.cc/2U7C-565N].
[73]. See generally First Nations in Canada, Gov’t of Can., https://www.rcaanc-cirnac.gc.ca/eng/1307460755710/1536862806124 [https://perma.cc/WN4N-FUWL].
[74]. See Sandro Galea et al., supra note 69, at 817.
[78]. See Medicare Telemedicine Health Care Provider Fact Sheet, Ctrs for Medicare & Medicaid Servs. (Mar. 17, 2020), https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet [https://perma.cc/9LEA-3QXS].
[80]. Ctrs. for Medicare & Medicaid Servs., COVID-19 Emergency Declaration Blanket Waivers for Health care Providers 1 (2020), https://www.cms.gov/files/document/summary-covid-19-emergency-declaration-waivers.pdf [https://perma.cc/4Y4E-GZUQ]. Blanket waivers may be issued during declared emergencies to ensure sufficient health care services are available to meet the needs of Medicare, Medicaid, and Child Health Insurance Program beneficiaries. Id. at 36. These waivers generally terminate no later than the end of the emergency period. Id. President Trump declared the coronavirus pandemic an emergency on March 13, 2020. Id.
[81]. Coronavirus Aid, Relief, and Economic Security Act, Pub. L. No. 116-136, § 3704, 134 Stat. 281, 416–17 (2020).
[82]. Ctrs. for Medicare & Medicaid Servs., Physicians and Other Clinicians: CMS Flexibilities To Fight COVID-19, at 1 (2020), https://www.cms.gov/files/document/covid-19-physicians-and-practitioners.pdf [https://perma.cc/NS86-VJG3].
[83]. Ctrs. for Medicare & Medicaid Servs., List of Services Payable Under the Medicare Physician Fee Schedule when Furnished via Telehealth, https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/Telehealth-Codes [https://perma.cc/4DVM-HSRG] (Oct. 14, 2020).
[84]. See 42 C.F.R. § 410.78(a)(3) (2020).
[85]. See Ctrs. for Medicare & Medicaid Servs., supra note 82, at 2.
[86]. Ctrs. for Medicare & Medicaid Servs., COVID-19 Frequently Asked Questions (FAQs) on Medicare Fee-for-Service (FSS) Billing 60 (2020) https://edit.cms.gov/files/document/medicare-telehealth-frequently-asked-questions-faqs-31720.pdf [https://perma.cc/TV58-8N8T].
[87]. Julia Hudman et al., How Private Insurers Are Using Telehealth to Respond to the Pandemic, Peterson-KFF Health Sys. Tracker (Aug. 6, 2020), https://www.healthsystemtracker.org/brief/how-private-insurers-are-using-telehealth-to-respond-to-the-pandemic [https://perma.cc/TZ3D-9KK2].
[88]. Substance Abuse & Mental Health Servs. Admin. et al., supra note 32, at 3.
[89]. Press Release, Indian Health Serv., IHS Receives More than $1 Billion for Coronavirus Response (Apr. 3, 2020), https://www.ihs.gov/newsroom/pressreleases/2020-press-releases/ihs-receives-more-than-1-billion-for-coronavirus-response [https://perma.cc/5UBJ-ZVEY].
[90]. Coronavirus Aid, Relief, and Economic Security Act, Pub. L. No. 116-136, § 3704, 134 Stat. 281, 416–17 (2020).
[92]. See Andy Joseph, Jr. et al., The National Tribal Budget Formulation Workgroup’s Recommendations on the Indian Health Service Fiscal Year 2021 Budget 14 (2019) https://www.nihb.org/docs/04242019/307871_NIHB%20IHS%20Budget%20Book_WEB.PDF [https://perma.cc/9X2F-WLAL].
[94]. Letter from Nat’l Cong. of Am. Indians et al. to Nancy Pelosi, Speaker, U.S. House of Representatives, and Kevin McCarthy, Minority Leader, U.S. House of Representatives, Re: COVID-19 Infrastructure Recovery Legislative Proposal (Phase #4) 17 (May 11, 2020), http://www.ncai.org/Covid-19/legislative-updates/C4_Tribal_Infrastructure_Priorities_-House-.pdf [https://perma.cc/QAR9-UVMD].