Aila Hoss**
I. Introduction
II. Federal Indian Law and Health Outcomes
III. Federal Indian Law and COVID-19
IV. The Structural Violence of Federal Indian Law in COVID-19 Response
Like countless other health conditions,[1] the COVID-19 pandemic has resulted in inequalities.[2] People of color are experiencing not only higher rates of COVID-19 infections[3] but also worse outcomes from the infection.[4] American Indians and Alaska Natives are experiencing COVID-19 infections at higher rates than other groups across several states including Arizona,[5] New Mexico,[6]and Wisconsin.[7] The Navajo Nation, in particular, has been adversely impacted by COVID-19. As of the 2010 census, Navajo citizenship is around 300,000 people[8] although more recent numbers cite citizenship population at over 350,000.[9] The Tribe has had over 10,780 cases with 571 deaths as of October 14, 2020.[10] By May 2020, the Navajo Nation had displaced New York City as having the highest per capita rates of COVID-19 infections in all the United States.[11]
This essay argues that, but for federal Indian law, American Indians and Alaska Natives would not have experienced the pervasive inequalities in COVID-19 response and health outcomes. It discusses the negative impact of federal Indian law on health outcomes generally before offering a specific discussion on the failures of federal Indian law in the context of the COVID-19 pandemic. It acknowledges the sad reality that the impact of these failures will continue to manifest in other forms, including trauma-related conditions.
Throughout the pandemic, Tribes have exercised their sovereignty and inherent public health authority to mitigate continued federal failings.[12] Some Tribal responses have been highly effective in preventing and mitigating outbreaks in their communities.[13] While these measures deserve both praise and profile, they are outside the scope of this paper, which instead focuses on federal law and policy.
II. Federal Indian Law and Health Outcomes
Tribal nations have exercised their sovereignty throughout what is now the continental United States and Alaska since time immemorial.[14] Colonization and genocide reduced the number of Tribes in existence.[15] Today, the United States recognizes the sovereignty of 574 Tribal nations,[16] although others still exist without the same legal status.[17] Sovereignty ensures the right of Tribes “to make their own laws and be ruled by them.”[18]
The United States relies upon unique laws and policies to navigate the federal-Tribal government relationships, which include tactics for assimilation, termination, and, more recently, increased efforts to support sovereignty.[19] The principles underlying these policies developed over the course of two hundred years and remain law today.[20] Federal Indian law is the body of law that defines the legal relationships between Tribes, states, and the federal government[21] in the context of treaty rights,[22] jurisdiction,[23] and economic development,[24] among other areas.[25] While this framework recognizes Tribal sovereignty, it also holds that Congress has plenary power to legislate regarding all matters concerning Indians,[26] allowing the federal government to preempt nearly all Tribal authority or rights guaranteed by treaty[27] if specifically authorized by Congress.[28]
Federal Indian law is a structural determinant of health.[29] These principles have undermined Tribal political and cultural sovereignty in a myriad of ways, including terminating recognition,[30] denying access to ancestral and sacred lands and waters,[31] denying rights to engage in cultural practices,[32] separating children and families from their Tribes,[33] among countless others. These adverse legal impacts perpetuate adverse health outcomes (Figure 1).[34] Namely, the trauma caused by these adverse legal decisions has created a “collective emotional and psychological injury both over the life span and across generations resulting from the history of difficulties that [Indians] as a group have experienced in America.”[35]
Health conditions linked to such historical trauma include depression, suicide, anxiety, disordered eating, commercial tobacco use, lack of contraception use,[36] and substance use disorder.[37] It is also correlated with higher Adverse Childhood Experience scores,[38] which is similarly associated with various health conditions including obesity[39] and substance use disorder.[40] The application of federal Indian law principles in today’s COVID-19 pandemic is also linked to health inequalities, as discussed below.
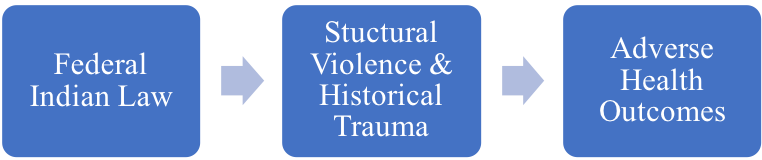
Figure 1: Logic Model Linking Federal Indian Law to Adverse Health Outcomes[41]
III. Federal Indian Law and COVID-19
Today’s application of federal Indian law perpetuates the adverse health outcomes ravaging through parts of Indian country. While Tribal programming has seen much success in filling gaps in federal programming,[42] this does not absolve the federal government of its treaty obligations. From water to health care, federal law has created the landscape that has disadvantaged Tribal communities. Only a small sample of examples are provided here.
One of the most obvious and well-documented failures in federal Indian health policies is the chronic underfunding of Indian health.[43] Numerous treaties between Tribes and the United States establish the legal obligation for the federal government to provide health care to American Indians and Alaska Natives.[44] This obligation is further memorialized in statutes and case law.[45] Despite these requirements, federal health care per capita spending for American Indians and Alaska Natives has been at a fraction of what is spent nationwide: $2,834 versus $9,990 in 2016 and $3,332 versus $9,207 in 2017.[46] Indian Health Service’s (IHS) budget meets little more than half of the health care needs in Indian country.[47]
Another striking example is the precarious funding for the Special Diabetes Program for Indians (SDPI). SDPI was established in 1997 to reduce diabetes disparities facing American Indians and Alaska Natives.[48] SDPI offers funding to over 400 programs supporting American Indians and Alaska Native communities[49] and has been viewed as incredibly successful.[50] Yet, funding for SDPI has repeatedly been at risk of lapsing and avoided by temporary fixes rather than permanent reauthorization.[51] At present, funding will lapse December 2020.[52] Individuals with diabetes are more likely to experience serious complications from COVID-19.[53] American Indians and Alaska Native experience diabetes at higher rates than other groups,[54] making COVID-19 particularly dangerous for Tribal communities.
Under the Robert T. Stafford Disaster Relief and Emergency Assistance Act (“Stafford Act”),[55] the president can declare a major disaster or emergency when an event overburdens Tribes, states, local governments, or territories,[56] which in turn allows these jurisdictions to secure additional resources and funding from the federal government.[57] Yet, receiving funding through the Stafford Act requires cost sharing by the governments receiving those funds.[58] Tribes are not exempted from this cost-sharing requirement, even for resources to respond to public health crises.[59]
The gaps in federal health care programming are particularly striking in the wake of the COVID-19 pandemic. For example, there have been issues with access to personal protective equipment for health care workers. The federal government supplied faulty masks to IHS facilities in the southwest.[60] IHS facilities quickly depleted necessary medical equipment, including ventilators and testing kits, early in the spring.[61] IHS only has thirty-three intensive care unit beds, and its physical space capacity is only has fifty percent of what is needed for the American Indian and Alaska Native population.[62] As another example, Tribal government access, and even IHS access to the Strategic National Stockpile, a stockpile of medicines, vaccines, and medical devices for use in public health emergencies,[63] is limited and not guaranteed.[64]
Federal Indian law requires that the United States maintain a trust responsibility towards Tribes.[65] The trust responsibility is a “fiduciary obligation . . . to protect tribal treaty rights, lands, assets, and resources, as well as a duty to carry out the mandates of federal [Indian] law.”[66] It also includes a requirement that federal agencies consult with Tribes prior to taking action that would impact Tribal communities.[67] Lack of federal consultation or inadequate consultation on Indian health policies is also pervasive.[68] For example, the federal government failed to consult with Tribes when allowing states to implement Medicaid work requirements[69] and when closing an emergency room.[70]
Underreporting population counts and failure to include American Indians and Alaska Natives in public health surveillance also put Tribal communities at a disadvantage. The Choctaw Nation leadership recently discussed the impact of census underreporting on federal COVID-19 relief funds.[71] The Tribe stated that it had lost out on tens of millions of dollars in COVID-19 relief and other program funding due to census underreporting.[72] Racial misclassification, omission of American Indians and Alaska Natives, and refusal to share public health data is already commonplace.[73] These issues are exacerbated during a pandemic,[74] particularly when the federal government refuses to provide COVID-19 data to Tribal Epidemiology Centers.[75] The Centers for Disease Control and Prevention is already obligated to provide this data under the Indian Health Care Improvement Act.[76] Lack of quality public health data can be particularly harmful because it makes it more difficult to identify outbreaks and highlight disparities. In turn, it makes it more difficult to identify appropriate policy solutions or justify additional policy action or funding.
Federal Indian policies have allowed for inadequate water access in many parts of Indian country. A spring 2020 study of reservation lands found that lack of indoor plumbing and potable water was linked to higher COVID-19 infection rates.[77] It is hardly surprising that a respiratory illness that can be prevented with frequent handwashing.[78] Navajo Nation lands include over 27,000 square miles[79] with over 170,000 people living on the reservation.[80] Over thirty percent of residents do not have access to running water.[81] Federal law has allowed for the continued diversion of limited water resources away from Tribal lands, exacerbating the current health crisis.[82]
IV. The Structural Violence of Federal Indian Law in COVID-19 Response
Structural violence is “invisible, embedded in ubiquitous social structures, normalized by stable institutions and regular experience.”[83] It “occurs whenever people are disadvantaged by political, legal, economic, or cultural traditions.”[84] As previously argued, federal Indian law perpetuates structural violence on American Indian and Alaska Native communities by establishing legal norms that disadvantage these communities in a variety of areas, including health.[85] In the context of the COVID-19 pandemic, this is all too clear.
The application of federal Indian law has allowed for the chronic underfunding of IHS and other health care programming; lack of and inadequate Tribal consultation; lack of access to sufficient personal protective equipment for Tribes and health care providers working in Indian country; inadequate access to public health data; inadequate access to water; among so many other issues not highlighted in this paper. By allowing the federal government to renege on its treaty and trust obligations, federal Indian law has perpetuated structural violence. It has normalized these conditions and normalized the adverse health outcomes for American Indians and Alaska Natives, namely higher rates of COVID-19 infections, complications, and deaths. Figure 2 outlines the connections between federal Indian law, structural violence, and COVID-19 outcomes.
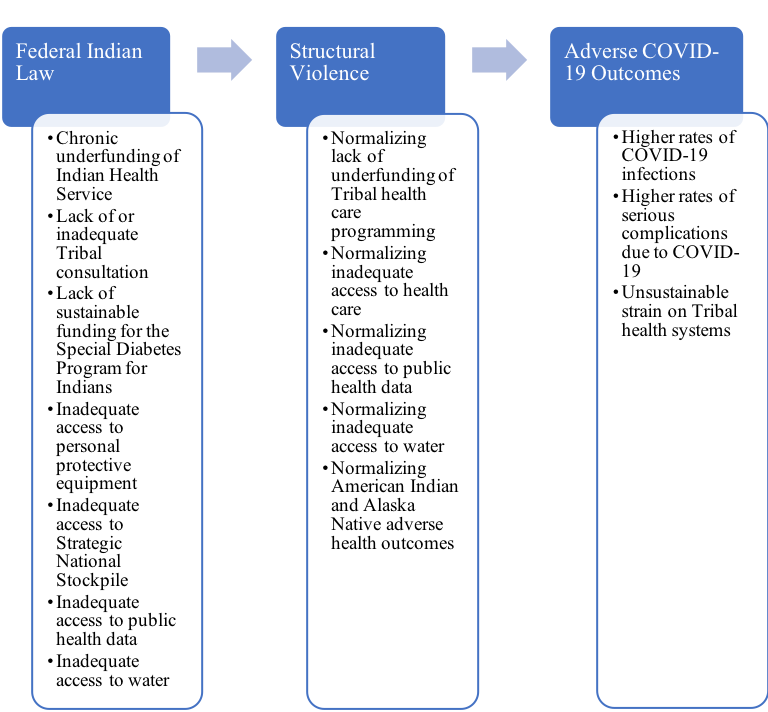
Figure 2: Logic Model Linking Federal Indian Law to Adverse COVID-19 Outcomes[86]
Federal Indian law should not be used as a tool to perpetuate health harm but instead should be used to support American Indian and Alaska Native health. How can this be done? Federal legislation can offer sufficient appropriations for Indian health care; permanent reauthorization of the SDPI; and guaranteed access to the Strategic National Stockpile. Federal agencies, without any legislation, can easily facilitate data sharing with Tribes and Tribal-serving organizations, provide more robust opportunities for consultation, and can structure funding opportunities to allow for increased funding to Tribes.
The suffering and death of Native people due to COVID-19 should not be normalized. The trauma of this suffering extends beyond the individuals and their family to the entire community and will have its own short-term and long-term health impacts. So, we are long overdue for the federal government to honor its treaty and trust obligations in all areas, including health.
* This paper was published in November 2020 during the COVID-19 pandemic. All dates and time descriptions refer to the 2020–21 COVID-19 pandemic unless otherwise stated.
** Aila Hoss is an Assistant Professor of Law at the University of Tulsa. Her research explores topics in public health law and the impact of federal Indian law on health outcomes. The author thanks Julie Combs for her research assistance. The author also thanks the student editors of the Arizona State Law Journal for excellent editorial assistance. This research was funded by a University of Tulsa College of Law Summer Research Grant.
[1]. See generally Ctrs. Disease Control & Prevention, CDC Health Disparities and Inequalities Report—United States, 2013, 62 Morbidity & Mortality Wkly. Rep., Nov. 22, 2013.
[2]. COVID-19 Cases by Race/Ethnicity, Kaiser Fam. Found., https://www.kff.org/other/state-indicator/covid-19-cases-by-race-ethnicity/ [https://perma.cc/3XYG-6HMC]; Hollie Silverman, Konstantin Toropin, Sara Sidner & Leslie Perrot, Navajo Nation Surpasses New York State for the Highest Covid-19 Infection Rate in the US, CNN (May 18, 2020, 5:55 PM), https://www.cnn.com/2020/05/18/us/navajo-nation-infection-rate-trnd/index.html [https://perma.cc/GM8L-Y4H9].
[3]. See Kaiser Fam. Found., supra note 2.
[4]. Taylor McNeil, Why People of Color Are Suffering More from COVID-19, Tufts Now (July 10, 2020), https://now.tufts.edu/articles/why-people-color-are-suffering-more-covid-19 [https://perma.cc/A5FP-92X8].
[5]. Emma Gibson, Analysis: Native Americans Infected with COVID-19 at Higher Rates in Arizona, Ariz. Pub. Media (July 10, 2020), https://news.azpm.org/p/coronavirus/2020/7/10/176298-analysis-native-americans-infected-with-covid-19-at-higher-rates-in-arizona/ [https://perma.cc/QQ3M-2FVM].
[6]. Elise Kaplan & Theresa Davis, ‘Huge Disparity’ in COVID-19 Death Rates for Native Americans in NM, Albuquerque J. (May 31, 2020, 12:05 AM), https://www.abqjournal.com/1461218/huge-disparity-in-covid19-death-rates-for-native-americans-in-nm.html [https://perma.cc/469Q-8KV7].
[7]. Danielle Kaeding, Health Disparities Leave Native Americans More Vulnerable to COVID-19, Wis. Pub. Radio (July 13, 2020, 6:30 AM), https://www.wpr.org/health-disparities-leave-native-americans-more-vulnerable-covid-19 [https://perma.cc/TJ6E-HDP3].
[8]. Navajo Div. of Health & Navajo Epidemiology Ctr., Navajo Population Profile 2010 U.S. Census 5 (2013), https://www.nec.navajo-nsn.gov/Portals/0/Reports/NN2010PopulationProfile.pdf [https://perma.cc/J42M-MK84].
[9]. Mona Gable, As Covid-19 Tears Through Navajo Nation, Young People Step Up To Protect Their Elders, Stat News (May 26, 2020), https://www.statnews.com/2020/05/26/navajo-nation-covid-19-youth-response-elders-health/ [https://perma.cc/T2ZJ-BRC2].
[10]. Dikos Ntsaaígíí-19 (COVID-19), Navajo Dep’t of Health, https://www.ndoh.navajo-nsn.gov/COVID-19 [https://perma.cc/UP72-WUTY] (Oct. 14, 2020).
[11]. Silverman, supra note 2.
[12]. See, e.g., South Dakota Tribe Sues Feds To Keep COVID-19 Checkpoints, ABC News (June 24, 2020, 2:31 PM), https://abcnews.go.com/Health/wireStory/south-dakota-tribe-sues-feds-covid-19-checkpoints-71437306 [https://perma.cc/3CMM-T6UF]; Lynda V. Mapes, Washington State Tribes, Allies Mobilize To Gather Medical Protection Needed in Coronavirus Fight, Seattle Times (Apr. 4, 2020, 7:48 PM), https://www.seattletimes.com/seattle-news/washington-state-tribes-allies-mobilize-to-gather-medical-protection-needed-in-coronavirus-fight/ [https://perma.cc/B7AX-Q5F6]; Patty Talahongva, Dean Seneca: ‘Optimistic’ Tribes Are Stepping Up to the Plate During Pandemic, Indian Country Today (Aug. 12, 2020), https://indiancountrytoday.com/newscasts/dean-seneca-optimistic-tribes-are-stepping-up-to-the-plate-during-pandemic-iC-5HSwNU0qBF9G7qxaUtw [https://perma.cc/K8NM-K35N].
[13]. Aila Hoss & Heather Tanana, Upholding Tribal Sovereignty and Promoting Tribal Public Health Capacity During the COVID-19 Pandemic, in Assessing Legal Responses to COVID-19 Report 77, 77–79 (Public Health Law Watch, Aug. 2020), https://static1.squarespace.com/static/5956e16e6b8f5b8c45f1c216/t/5f445c11d10a1b0c4024a9c9/1598315537385/Chp10_COVIDPolicyPlaybook-Aug2020.pdf [https://perma.cc/GC82-5RCF]. For examples off Tribal efforts to respond to the COVID-19 pandemic, see, e.g., Kewa Pueblo (New Mexico), Indianz.com (Aug. 11, 2020), https://www.indianz.com/covid19/?p=7781 [https://perma.cc/WA5Q-SGRM]; Nina Lakhani, Native American Tribe Takes Trailblazing Steps To Fight Covid-19 Outbreak, Guardian (Mar. 18, 2020, 1:25 PM) https://www.theguardian.com/us-news/2020/mar/18/covidcoronavirus-native-american-lummi-nation-trailblazing-steps [https://perma.cc/6H4D-B283].
[14]. Stephen L. Pevar, The Rights of Indians and Tribes 81 (Oxford Univ. Press 4th ed. 2012).
[15]. Roxanne Dunbar-Ortiz, An Indigenous Peoples’ History of the United States 41, 59 (Bos.: Beacon Press 2014).
[16]. Indian Entities Recognized By and Eligible To Receive Services from the United States Bureau of Indian Affairs, 85 Fed. Reg. 5462, 5462 (Jan. 30, 2020).
[17]. Martha Salazar, State Recognition of American Indian Tribes, 24 Nat’l Conf. of State Legis. (2016), https://www.ncsl.org/research/state-tribal-institute/state-recognition-of-american-indian-tribes.aspx [https://perma.cc/W6L2-A846].
[18]. Williams v. Lee, 358 U.S. 217, 220 (1959).
[19]. See, e.g., Robert J. Miller, The History of Federal Indian Policies 14–18 (Mar. 17, 2010) (unpublished manuscript), https://papers.ssrn.com/sol3/papers.cfm?abstract_id=1573670 [https://perma.cc/CJQ5-AJU4].
[20]. Cohen’s Handbook of Federal Indian Law § 1.01 (Nell Jessup Newton ed., 2012) [hereinafter Cohen’s Handbook].
[21]. Matthew L.M. Fletcher, Federal Indian Law § 3 (W. Acad. Publishing, 1st ed. 2016).
[23]. Cohen’s Handbook, supra note 20, § 7.
[25]. Fletcher, supra note 21, §§ 3, 9
[26]. United States v. Kagama, 118 U.S. 375, 384–85 (1886); Ex Parte Crow Dog, 109 U.S. 556, 572 (1883).
[27]. Kagama, 118 U.S. at 383–85.
[29]. Aila Hoss, Federal Indian Law as a Structural Determinant of Health, 47 J.L. Med. & Ethics 34, 34 (2019).
[30]. Pevar, supra note 14, at 271–74.
[31]. See, e.g., South Dakota v. Yankton Sioux, 522 U.S. 329, 357–58 (1998); Hagen v. Utah, 510 U.S. 399, 418–19 (1994); Nevada v. United States, 463 U.S. 110, 145 (1983); Montana v. United States, 450 U.S. 544, 556–57 (1981).
[32]. Matthew L.M. Fletcher, Looking to the East: The Stories of Modern Indian People and the Development of Tribal Law, 5 Seattle J. Soc. Just. 1, 3–5 (2006); Lyng v. Nw. Indian Cemetery Protective Ass’n, 485 U.S. 439, 457–58 (1988); Navajo Nation v. U.S. Forest Serv., 535 F.3d 1058, 1062–63 (9th Cir. 2008).
[33]. Robert Laurence, Indian Education: Federal Compulsory School Attendance Law Applicable to American Indians: The Treaty-Making Period: 1857-1871, 5 Am. Indian L. Rev. 393, 401 (1977); Indian Relocation Act of 1956, Pub. L. No. 84-959, 70 Stat. 986.
[34]. Hoss, supra note 29, at 37.
[35]. Peggy Halpern, Obesity and American Indians/Alaska Natives 31 (2007) (citing Edna Steinman, Native Americans Suffer from ‘Historical Trauma,’ Researcher Says, United Methodist Church News (July 27, 2005)).
[36]. Joseph P. Gone et al., The Impact of Historical Trauma on Health Outcomes for Indigenous Populations in the USA and Canada: A Systematic Review, 74 Am. Psych. 20, 27–28 (2019).
[37]. See, e.g., Maria Yellow Horse Brave Heart, The Historical Trauma Response Among Natives and its Relationship with Substance Abuse: A Lakota Illustration, 35 J. Psychoactive Drugs 7, 7 (2003); Monica C. Skewes & Arthur W. Blume, Understanding the Link Between Racial Trauma and Substance Use Among American Indians, 74 Am. Psych. 88, 88 (2019).
[38]. Dolores Subia BigFoot et al., Honoring Children: Treating Trauma and Adverse Childhood Experiences in American Indian and Alaska Native Communities, Am. Psych. Ass’n (Nov. 2018), https://www.apa.org/pi/families/resources/newsletter/2018/11/native-american-trauma [https://perma.cc/PY5N-BKDS].
[39]. Bernard F. Fuemmeler et al., Adverse Childhood Events Are Associated with Obesity and Disordered Eating: Results from a U.S. Population-Based Survey of Young Adults, 22 J. Traumatic Stress 329, 329 (2009).
[40]. Substance Abuse & Mental Health Servs. Admin., The Role of Adverse Childhood Experiences in Substance Abuse and Related Behavioral Health Problems 1, https://www.cambridgema.gov/CDD/Projects/Planning/~/media/328D3B716A24449D8504357BD3865949.ashx [https://perma.cc/R6N3-GVFU]; see also Teresa N. Brockie et al., The Relationship of Adverse Childhood Experiences to PTSD, Depression, Poly-Drug Use and Suicide Attempt in Reservation-Based Native American Adolescents and Young Adults, 55 Am. J. Cmty. Psych. 411 (2015).
[41]. Hoss, supra note 29, at 37.
[42]. See Fact Sheet: Tribal Self-Governance, Indian Health Serv. (July 2016), https://www.ihs.gov/newsroom/index.cfm/factsheets/tribalselfgovernance/ [https://perma.cc/S7J9-9QE8].
[43]. U.S. Comm’n on C.R., Broken Promises: Continuing Federal Funding Shortfall for Natives Americans 6 (2018); Neill F. Piland & Lawrence R. Berger, The Economic Burden of Injuries Involving American Indians and Alaska Natives: A Critical Need for Prevention, 32 IHS Primary Care Provider 269, 270 (2007).
[44]. Cohen’s Handbook, supra note 20, § 22.04.
[45]. See, e.g., Indian Health Care Improvement Act of 1976, Pub. L. No. 94-437, 90 Stat. 1400 (1976); Rosebud Sioux Tribe v. United States, 450 F.Supp.3d 986, 996 (D.S.D. 2020).
[46]. U.S. Comm’n on C.R., supra note 43, at 66–67.
[48]. SDPI Overview, Nat’l Indian Health Bd., https://www.nihb.org/sdpi/sdpi_overview.php [https://perma.cc/EHX5-DNXP].
[50]. See, e.g., Local Impact—Alabama, Nat’l Indian Health Bd., https://www.nihb.org/sdpi/local_impact_poarch_creek.php [https://perma.cc/BZ7N-66B6]; Special Diabetes Program for Indians (SDPI): Mitigating COVID-19 Risk, Urb. Indian Health Inst. (June 8, 2020), https://www.uihi.org/resources/special-diabetes-program-for-indians-sdpi-mitigating-covid-19-risk/ [https://perma.cc/2BU9-28DG].
[51]. See Latest Legislative Updates: SDPI Renewed Through November 21, 2019, Nat’l Indian Health Bd. (Oct. 2, 2019), https://www.nihb.org/sdpi/legislative_updates.php [https://perma.cc/JQ92-F8WP].
[52]. 42 U.S.C. § 254c-3(c)(2)(D).
[53]. How COVID-19 Impacts People with Diabetes, Am. Diabetes Ass’n, https://www.diabetes.org/coronavirus-covid-19/how-coronavirus-impacts-people-with-diabetes [https://perma.cc/Z8YG-WKHD].
[54]. Native Americans with Diabetes, Ctrs. for Disease Control & Prevention (Jan. 10, 2017), https://www.cdc.gov/vitalsigns/aian-diabetes/index.html [https://perma.cc/4DJ4-LAWR].
[55]. Robert T. Stafford Disaster Relief and Emergency Assistance Act of 1974, Pub. L. No. 93-288, 88 Stat. 143 (codified as amended at 42 U.S.C. §§ 5121–5206 and various sections of titles 12, 16, 20, 26, and 38 of the United States Code).
[56]. 42 U.S.C. §§ 5170(a), 5191(b).
[57]. 42 U.S.C §§ 5170(a), 5192(a)(1)–(8).
[60]. Yeganeh Torbati & Derek Willis, The Feds Gave a Former White House Official $3 Million To Supply Masks to Navajo Hospitals. Some May Not Work., ProPublica (May 22, 2020, 4:10 PM), https://www.propublica.org/article/the-feds-gave-a-former-white-house-official-3-million-to-supply-masks-to-navajo-hospitals-some-may-not-work [https://perma.cc/5T7Z-2F2M].
[61]. Letter from Nat’l Indian Health Board et al. to Nancy Pelosi, Speaker, U.S. House of Reps., and Kevin McCarthy, Minority Leader, U.S. House of Reps. 1 (Apr. 8, 2020), https://www.nihb.org/covid-19/wp-content/uploads/2020/04/FINAL_HOUSE_ATTACHMENT-2_NIHB_-Phase-4-Tribal-Healthcare_Public-Health-Priorities.pdf [https://perma.cc/3WX2-8ZUN].
[63]. Strategic National Stockpile, Pub. Health Emergency, https://www.phe.gov/about/sns/Pages/default.aspx [https://perma.cc/AT5Y-HZT2].
[64]. Press Release, Rep. Kendra Horn, Rep. Horn Introduces Bipartisan Bill To Guarantee Tribal Health Authorities Access to Strategic National Stockpile (Mar. 23, 2020), https://horn.house.gov/news/documentsingle.aspx?DocumentID=199 [https://perma.cc/RE4J-J3NC].
[65]. See, e.g., United States v. Mitchell, 445 U.S. 535, 536–37 (1980); Menominee Tribe of Indians v. United States, 391 U.S. 404, 408–09 (1968); Joint Tribal Council of the Passamaquoddy Tribe v. Morton, 528 F.2d 370, 380 (1st Cir. 1975).
[66]. Frequently Asked Questions: What Is the Federal Indian Trust Responsibility?, U.S. Dep’t. of the Interior, Bureau of Indian Affs., http://www.bia.gov/FAQs/index.htm [https://perma.cc/AVL9-4YRU].
[67]. Memorandum on Government-to-Government Relations with Native American Tribal Governments, 59 Fed. Reg. 22951, 22951 (Apr. 29, 1994).
[68]. See, e.g., Pevar, supra note 14, at 43–44.
[69]. Dan Diamond, Trump Challenges Native Americans’ Historical Standing, Politico (Apr. 22, 2018, 7:07 AM), https://www.politico.com/story/2018/04/22/trump-native-americans-historical-standing-492794 [https://perma.cc/64R3-ZSD2].
[70]. Yankton Sioux Tribe v. U.S. Dep’t of Health & Human Servs., 533 F.3d 634, 637 (8th Cir. 2008).
[71]. Talli Nauman, Native Sun News Today: Tribes Jump on Census Bandwagon, Indianz.com (Aug. 7, 2020),
https://www.indianz.com/News/2020/08/07/native-sun-news-today-tribes-jump-on-cen.asp [https://perma.cc/AEN9-TK6U].
[73]. See Tribal Epidemiology Ctrs., Best Practices in American Indian & Alaska Native Public Health 18–123 (2013) (listing the parent organizations of the TECs).
[74]. Emma Whitford, Navajo Virus Case Bump Highlights Data Challenges, Law360 (May 15, 2020, 12:50 PM), https://www.law360.com/articles/1273585/navajo-virus-case-bump-highlights-data-challenges [https://perma.cc/2E6F-G8Z9].
[75]. Letter from Martin Heinrich, Sen., U.S. Senate, to Robert Redfield, Director, Ctrs. for Disease Control & Prevention (June 18, 2020), https://www.heinrich.senate.gov/download/?id=04654AA9-B1DF-41F7-ADE8-04722C2B89CE&download=1 [https://perma.cc/P7Z3-XMTB].
[76]. 25 U.S.C. § 1621m(c), (e)(2).
[77]. Desi Rodriguez-Lonebear et al., American Indian Reservations and COVID-19: Correlates of Early Infection Rates in the Pandemic, 26 J. Pub. Health Mgmt. & Prac. 371, 371 (2020).
[78]. Hand Hygiene Recommendations, Ctrs. for Disease Control & Prevention, https://www.cdc.gov/coronavirus/2019-ncov/hcp/hand-hygiene.html [https://perma.cc/8KR6-9F73] (May 17, 2020).
[79]. History, Navajo Nation, https://www.navajo-nsn.gov/history.htm [https://perma.cc/GEC9-U9EA].
[80]. Navajo Div. of Health & Navajo Epidemiology Ctr., supra note 8, at 13.
[81]. Andrew Curley, Contested Water Settlements Inflamed the Navajo Nation’s Health Crisis, High Country News (Aug. 11, 2020), https://www.hcn.org/articles/indigenous-affairs-water-contested-water-settlements-inflamed-the-navajo-nations-health-crisis [https://perma.cc/RDR9-P2QL].
[83]. Deborah Du Nann Winter & Dana C. Leighton, Structural Violence, in Peace, Conflict, and Violence: Peace Psychology in the 21st Century 99 (Christie, Wagner & Winter eds., 2001).
[85]. Aila Hoss, A Framework for Tribal Public Health Law, 20 Nev. L.J. 113, 133 (2019).